

The Sex and Gender Health Education Summit is a national collaboration brought together by the American Medical Women’s Association, the Laura W. Bush Institute for Women's Health at Texas Tech University Health Science Center, Mayo Clinic, and Thomas Jefferson University along with other national supporters.
The three-day event, which runs from September 11 -13, will provide attendees with a road map for integrating sex and gender-based medicine into medical and health professions education, while providing an opportunity for attendees to interact with leaders across different healthcare professions, including and not limited to: medicine, nursing, dentistry, occupational therapy, pharmacy, physical therapy, advanced practitioners including physician assistants and nurse practitioners, behavioral health, emergency medical technicians, and others.
The 2020 Sex and Gender Health Education Summit will:
*Highlight innovative and sustainable curriculum methods for teaching sex and gender specific health *Create a network to support and progress the integration of sex and gender differences into health professionals’ education *Expand multi-disciplinary opportunities by convening leaders from across different healthcare professionsThe 2020 Summit will build upon the momentum from the prior summits and expand multi-disciplinary opportunities. The goal is to support and progress the integration of sex and gender differences into health professionals’ education through innovative and sustainable curriculum methods.
-

Inclusivity in Action: Interprofessional Curricula Integrates Two-Step Question for Sex and Gender Identity
N. Ankam, MD; A. B. Mitchell; K. A. Bell; R. Hass; and A. M. Lopez
Background: Identifcation of sex and gender identity is the first step to inclusive care for sex and gender minorities, and studies have shown that health care providers may make heteronormative assumptions about sex and gender. Implemented in 2007, the Jefferson Health Mentors Program (JHMP) involves firstand second-year students from couple and family therapy, human genetics and genetic counseling, medical laboratory sciences, medicine, nursing, occupational therapy, pharmacy, physical therapy, and physician assistant studies. In the First assignment, 140 student teams complete a comprehensive questionnaire, the Individual Life and Wellness History with their Health Mentor. Health Mentors live with one or more chronic conditions and range in age from 27 to 95 years old, with the majority over age 50. Interprofessional education where students learn from, with, and about each other is an ideal place for students to be exposed to the sex and gender two-step question.
Objectives: To describe our experience with 713 students involved in the JHMP asking the two-step sex and gender question.
Methods/Research: In Fall 2018, the two-step sex and gender question was added to the questionnaire. The module evaluation included both a quantitative and a qualitative question to gather student feedback on the inclusion of the two-step sex and gender questions. The qualitative responses were reviewed for themes, and the authors came to consensus.
Conclusions/Impact: Common themes included student appreciation of the importance of the questions; confusion of the Health Mentors with the questions; student perception of generational differences, and student teams having no issues with the questions. No Health Mentors dropped out of the program after the First assignment, other than those who dropped out for health related reasons. Interprofessional education can provide a venue for normalizing the two-step sex and gender question.
-

IM with Her: Fostering Career Advancement of Female Internal Medicine Residents
S. Bharel, Michelle Hannon, K. Duffey, R. Redffeld, A. Greidinger, R. Onyeali, and G. Diemer
Background: Despite the rising number of matriculating female medical students, a gender gap favoring men exists in multiple arenas within academic medicine. Prior studies suggest that gender-specifc professional networking groups increase the likelihood of women attaining leadership positions.
Objectives: Our goal was to create a multidisciplinary group with a flat hierarchy within the Internal Medicine Department in order to foster mentorship, sponsorship, allyship, and scholarship to ultimately improve professional advancement opportunities for female internal medicine residents.
Methods/Research: A group named “IM with Her” was created at Thomas Jefferson University Hospital in July 2018. IM with Her is composed of internal medicine residents and faculty of all genders. The group has hosted monthly onehour conferences called “Monday Mentors” that pair a resident with a faculty member to host a discussion surrounding a topic of their choosing related to adversity and disparity faced by female physicians. Additionally, the group has held periodic evening sessions discussing topics such as salary and contract negotiation.
Conclusions/Impact: The IM with Her group has made significant progress toward its goals. The pairing of a resident and faculty member for Monday Mentors discussions allows for one-on-one mentorship regarding both personal and professional topics. These sessions also provide dedicated time for networking amongst residents and faculty, facilitating sponsorship and allyship. Additionally, the sessions often lead to further initiatives spearheaded by IM with Her members including scholarly projects and examinations of institutional policies (for example those surrounding sexual harassment and lactation room accessibility). In the future, IM with Her will focus on continuing to foster mentorship, sponsorship, and allyship, on advancing research related to gender disparities in medicine, and on developing institutional changes.
-

Success of a Student Organized Gender and Sexuality Seminar Series
C. Briskin, M. R. Kasoff, J. Mahabamunge, K. R. Morel, J. Budrow, C. B. Hart, S. Spiegel, D. Risucci, and J. Koestler
BACKGROUND: The lack of medical school education on lesbian, gay, bisexual, andtransgender (LGBT) health contributes to explicit and implicit bias anddiscrimination against LGBT patients. This results in health disparities amonggender and sexual minority (GSM) populations and can lead to worse healthoutcomes. New York Medical College students organized a Gender and Sexuality inMedicine seminar series to increase medical student education, reduce bias, andultimately, improve patient outcomes.
OBJECTIVES: This study aims to improve medical student uency in sex, gender,and reproductive health and prepare medical students to treat LGBT patients in acompassionate and knowledgeable way.
METHODS/RESEARCH: We advertised a Gender and Sexuality in Medicine seminar series to medical students via email and asked all participants to completean anonymous online pre-course survey. Content area experts presented seminarson PrEP/HIV, LGBT mental health, and puberty suppression in transgenderchildren, among other topics. Students then completed an anonymous online post-course survey to assess the eectiveness of individual lectures and the seminarseries overall.
CONCLUSIONS/IMPACT: 59 first and second year medical students completedthe lecture series, with 76% of attendees identifying as female and 24% identifying as male. This illustrates strong student interest in and demand for education onthese topics, particularly amongst female students. Additionally, attendeesexpressed an increased level of comfort in their ability to ask patients questionsregarding gender and sexuality. The largest increase in comfort was for recognizingfemale genital cutting, counseling patients on HIV prevention, and discussingsexual violence with patients. High lecture satisfaction ratings, voluntary student participation, and increases in comfort level indicate the series was effective in addressing health disparities among GSM patients. This also suggests GSM topicsshould be integrated into the standard preclinical curriculum.
-

Bridging the gap: Increasing awareness of sex differences in opioid addiction using social media platforms
Yuwen Cheng, BA; N. Khatchadourianm MPH; J. Esguerra, MA; E. Seeley, BSE; Y. Abushukur; M. Feldman; E. Randall, BS; and C. Cheah, MD
HONORABLE MENTION
Background: Current efforts to combat the opioid epidemic in the United States do not take into account the sex differences in opioid response, prescription, use, and addiction. There is a need for medical professionals and the general public to understand these differences to properly prevent, address, and treat opioid addiction. Healthcare professionals and patients often use the Internet and social networking websites to access and share medical information. These platforms provide an innovative way to educate these groups on various topics in medicine. The American Medical Women’s Association (AMWA) created the Opioid Addiction in Women Task Force to positively impact care for women with opioid addiction.
Objectives: Increase health literacy surrounding sex differences in opioid addiction in the general public and healthcare providers via social media platforms
Methods/Research: The AMWA Opioid Task Force consists of physicians and medical students across the country who meet virtually each month. With guidance from supervising physicians, educational infographics, pamphlets, and videos are created to facilitate the dissemination of complex scientiffc data in a simple and engaging manner. Information is subsequently shared via social media platforms, such as Instagram, Twitter and YouTube, where they can be easily accessed by healthcare providers, medical students, and the public.
Conclusions/Impact: This is one of the few organizations with national exposure that highlights sex and gender differences in the opioid crisis and aims to increase health literacy for both the general public and health care providers. We have successfully distributed information regarding sex differences in opioid addiction during Women’s Health Week 2020 on the national AMWA website, Instagram, and Twitter. Our future plans include producing and sharing videos on YouTube about opioids, addiction, and pain management, especially in women. We hope to encourage current and future physicians to initiate discussions surrounding sex/gender-speciffc health, speciffcally in opioid addiction.
-

The Great Gender Divide: Gender-related discrepancies of N95 mask protection
Laura E. Christopher, BS and T. M. Rohr-Kirchgraber, MD, FACP, FAMWA
Background: During the COVID-19 pandemic, healthcare professionals are at increased risk of transmission due to their direct contact with infected patients. To ensure protection, properly fitting personal protective equipment (PPE) must be worn. N95 respirator masks are a component of PPE outlined by the CDC for COVID-19; however, N95 masks do not offer protection if they do not fit properly. Fit testing is performed to ensure adequate seal of the mask and proper fit.
Objective: The objective of this project was to attempt to identify a gender-related difference in fittesting failure rates.
Methods: A single institutional retrospective review was performed on individuals who underwent fit testing from December 2019 to June 2020. Two mask sizes were available for fit testing (Model 3M1860, Regular/Small). Fit test results were divided into two groups, male or female, and evaluated for failure rates. Reasons for fit test failures were noted as: large-boned, small-boned, facial asymmetry, facial hair, and/or no reason reported. Exclusion criterion included failure due to facial hair. Results: A total of 336 tests were performed during this period, with 31 exclusions for facial hair. Data analyzed included 305 total respirator fit test results: 110 male and 195 female. Females fail at signifcantly higher rates, 6.67%, compared to males, 2.27% (p=0.001). Specifcally, females failed due to being small-boned when compared to reasons for male fit testing failures (p<0.0001).
Conclusion: Gender-related differences in PPE fit is not new; however, the COVID- 19 pandemic has made the situation more acute. Females are faced with wearing masks that do not properly fit; N95 masks were not designed for female facial dimensions and because of inadequate fit, female healthcare workers are not properly protected. Developing a gender-specifc approach to designing N95 masks is vital in the upcoming months, as a potential second wave of COVID-19 is approaching.
-

Healthcare Professional Students' Attitudes, Beliefs, and Knowledge Regarding Transgender Healthcare
J. Clark, BS; P. Chung, MD; and A. Wolf, MD
Background: In our current medical system, transgender patients face discrimination and lack access to physicians competent in transgender specific health issues. Despite the fact that many medical schools and other healthcare professional schools are incorporating LGBT+ curriculum, research shows that many students still lack the skills and knowledge to comfortably care for the transgender patient population.
Objectives: To assess Thomas Jefferson University (TJU) healthcare professional students’ attitudes, beliefs, and knowledge regarding transgender health, and to assess students’ prior educational experiences and current educational preferences.
Methods: All students enrolled in one of the following colleges at TJU: health professions, nursing, pharmacy, population health, rehabilitation sciences, and medical school, were asked to participate in a 5-minute anonymous survey approved by IRB. Students were asked to answer questions about their attitudes, beliefs; comfort, skill, and knowledge level regarding transgender care along with any prior transgender health education and their educational preferences.
Results: There were a total of 337 responses with a response rate of 4.3%. Over 80% of students were interested in learning more about transgender healthcare issues. Less than 20% of students reported they lacked the skill and comfort level to adequately treat this patient population. 67% of students received some form of education regarding transgender healthcare issues with medical students reporting a signicantly high rate of 79.5% (p < 0.001). The majority felt it was successful in increasing knowledge (85%) comfort (85%), and skill level (63%). Participants wanted to practice skills with clinical skills session, standardized patient encounter, and clinical elective
Conclusion: Overall students at TJU feel they have a good base to adequately care for the transgender patient population; however, many students expressed interest in learning more about transgender specific health issues. A possible solution to this would be to provide more curricular opportunities with emphasis on practicing clinical skills
-

Creating a Medical Home for Trans Older Adults: Challenges, education, and best practices
Michael Danielewicz, MD; T. Hsiao, MS2; J. J. Liantonio, MD, MBA, MHDC; E. Collins, MD; B. E. Salzman, MD; and S. M. Parks, MD
Background: LGBT individuals face multiple disparities and challenges navigating the healthcare system. Most attention on such issues has focused on LGBT youth, leaving older adults as an especially vulnerable population. LGBT older adults are more likely than their heterosexual counterparts to experience poverty, worse mental and physical health, and mistreatment under current care models. Trans older adults represent a particularly underserved group and often have specialized care needs, including hormone therapy and behavioral healthcare. Geriatricians can help improve access to care with increased sensitivity toward and knowledge of LGBTspecific issues. With the unique challenges faced by LGBT older adults in mind, Jefferson Geriatrics, an outpatient practice devoted to the care of older adults, launched an initiative to create more LGBT-inclusive and trans-friendly primary care services in the Philadelphia region.
Objectives: After engaging with our poster, participants will: 1) Understand needs and challenges facing LGBT older adults, focusing on trans older adults 2) Identify best practices for providing trans-competent primary care 3) Explore concerns and challenges facing health care providers and staff in caring for a trans older adult population
Methods: An online survey was administered to healthcare providers and staff in a geriatric primary care practice to assess knowledge and attitudes related to LGBT individuals. Providers underwent cultural competency training pertaining to the care of the LGBT aging community. They also participated in medical competency training in areas such as HIV management and hormone therapy for trans individuals. Finally, a survey was conducted within an LGBT aging community to help gain an understanding of attitudes, perceptions and needs of older LGBT adults.
Conclusions/Impact: There remains much opportunity to improve upon the care of LGBT older adults, in particular trans older adults. In our poster, we describe a model for practice transformation to create a medical home for trans older adults.
-

Critical Content-A Novel Graduate Medical Education Intervention to Address Gender & Sexual Minority/Differences in Sexual Development Health
A. Filip, MD; E. Halpern, MD; and A. Waad, MA
Introduction & Background: Following directives from the Institute of Medicine 1 and AAFP 2 , we aimed to create an intervention for Family and Internal Medicine Residents to gain familiarity with gender and sexual minority (GSM) / differences in sexual development (health topics). Existing literature regarding GSM/DSD health training interventions does not provide topic based recommendations for instructing medical trainees within their chosen specialty. We aim to assess curricular content, applicability to medical practice, and subsequent attitudes and beliefs from trainees regarding readiness to interact with and treat GSM/DSD patients.
Methods & Framework: Internal Medicine ( IM ) and Family Medicine FM ) residents will participate in a three (3) hour workshop focusing on GSM/DSD health topics. Workshop content is curated based upon an assessment of current gaps in GSM/DSD education and professional development. Learning objectives for trainees were identified, and accompanying constructs were developed for later assessment of integration into professional practice. A semi structured protocol was also developed to collect qualitative reflections on the curriculum, as well as personal attitudes / beliefs regarding treatment of GSM/DSD patients. The assessment of the initial intervention was delayed due to COVID 19; this poster showcases the designed curriculum and its prospective assessment features.
Implementation & Assessment: COVID 19 posed unforeseen challenges, which barred us from assessing this intervention along its originally intended timeline. We intend to implement the invention in its entirety for the Fall 2020 cohort. We encourage others seeking to adopt this curriculum to utilize innovative assessment opportunities such as simulated patients or role plays to assess trainee progress toward learning outcomes. Pre and post assessment metrics will be collected from all trainees during the intervention’s Fall 2020 delivery. Semi structured focus groups will also be conducted. We will use analyses to inform further program development, content inclusion, and supplementary learning experiences to accompany the didactic curriculum. This module serves as a “starting point” for trainees’ continued education on GSM / DSD health topics. We recognize the need for continued expansion of content on marginalized LGBTQ+ communities.
-

Comparison of Sex Specific Data among Hospitalized Covid-19 Patients
J. Fleischer, BA; R. A. Pallay; and D. S. Corwin, MD
It is critical to identify factors that contribute to disease severity among patients diagnosed with COVID-19. A systematic review of sex specific COVID-19 clinical outcomes demonstrated that female patients have lower rates of severe infection and mortality. This study investigates the correlation between biological sex and predisposing conditions as well as COVID-19 disease severity among 689 patients hospitalized within the St. Luke’s Hospital Network in Eastern PA/Western NJ. The sample is comprised of 45.8% female participants, of whom 30.2% identify as Hispanic or Latino, and 57.9% identidied their race as caucasian. Mean age of participants is 64.0 years (+/- 16.7). Data was extracted from patients electronic medical records both during their admission and after discharge. Chi squared test of independence was performed to examine the relation between known COVID-19 risk factors and COVID-19 infected female patients (n=314) compared to male patients (n=373). Risk factors stratied by biological sex showed that female patients were more likely to have COPD (p < 0.05) and asthma (p < 0.001), and less likely to have smoke exposure (p < 0.05). There was no statistically significant difference in disease severity between the sexes with respect to intubation rate (p = 0.07) and mortality (p = 0.59). The results of this study are important to show that the trend of increased severity among males is not ubiquitous. Limitations of this study include small sample size, ongoing treatment protocol modifications with provider treatment bias, and overrepresentation of obesity.
-

Are State Policymakers Aware of Sex and Gender Impacts on Opioid Use Disorder?
T. Goss, MPH; C Newman, MD; J. Patrick-Esteve, MD, MSPH; J Esguerra, MA; and K. J. Templeton, MD
HONORABLE MENTION
Background: Sex and gender-based differences have been identified as risks for opioid use disorder (OUD) and treatment outcomes. In response to the “opioid crisis,” states have developed action plans to inform strategies of state agencies, impact legislative efforts, and help prioritize funding allocations for prevention initiatives, substance use disorder treatment, and law enforcement programs.
Objectives: This study aimed to provide the first analysis of state opioid action plans and their inclusion of gender-specific issues. The results of this study would be used to develop educational materials and programs for state policymakers to inform policy decisions and improve the care of women with OUD.
Methods: Forty-nine state action plans were identified from state websites and were analyzed for their inclusion of 15 variables covering provider education in gender differences, pregnancy-related topics, and discussion of gender-based differences in opioid addiction and treatment.
Results: Forty-one percent of states mentioned prenatal or postpartum care for women with OUD. Only 14% of states speciffcally mentioned pregnancy-related opioid use stigma, 12% mentioned contraceptive care/access, 8% mentioned family planning provider education, and 24% of states mentioned trauma-informed care. Three states mentioned gender differences in social risk factors, another three states mentioned treatment barriers specific to women, and only two states mentioned treatment stigma specific to women.
Conclusions: Few action plans contained gender-specific information; those that did focused almost exclusively on pregnancy and neonatal opioid withdrawal syndrome, showing a lack of understanding about the issues faced by women with OUD outside of reproductive health. Given the rising rate of opioid-related deaths among women and the impact of OUD on women of every age, state opioid policies need to be inclusive of the unique needs of women. This will require education of policymakers about gender-based differences in addiction physiology, medical and social risk factors, and barriers to treatment.
-

Effectiveness of an Educational Workshop on Dental Hygiene Students’ Competence and Comfort in Treating Transgender Patients
R. Handman, RDH, MDH, EdD
Background: Transgender individuals face barriers to health care, such as harassment, violence, and the refusal of care. Current literature shows a lack of instruction about caring for sexual minority patients in dental and allied dental education programs, which contributes to the barriers to care for this population.
Objective: The purpose of this quasi-experimental study was to determine the effectiveness of an educational workshop on dental hygiene student competence and comfort levels in treating transgender patients. Methodology Dental hygiene students’ competence and comfort levels in treating transgender individuals were evaluated using an adapted version of the Assessing Medical Attitudes Toward Transgender Care survey. The researcher collected primary data from a convenience sample of 45 dental hygiene students who attended an educational workshop about caring for transgender individuals. Data were collected at Week 1 (baseline) and Week 6 (post-workshop).
Results: The researcher used the Wilcoxon signed-rank test to analyze the data. The results showed a statistically significant increase from pretest to posttest in competence (1.6667 - 3.0000; z = 5.373) and comfort (3.0000 - 3.8000; z = 4.799) scores after attending the educational workshop, p<.05.
Conclusions: The findings of this study provide evidence that suggests education about transgender health care increases competence and comfort levels among dental hygiene students. Educators should consider including this content in dental and allied dental education curricula. When creating and revising dental hygiene curricula, educators and policymakers should ensure this content is included in suffcient scope and depth to prepare graduates to care for this population.
-

Investigating Gender Disparities in Internal Medicine Residency Awards
M. Hannon, MD; K. Duffey; S Bharel; A. Greidinger; E. Stewart; and G. Diemer
Background: Significant gender disparities persist in career advancement for physicians. Studies have highlighted the lack of female representation in awards from both academic institutions and professional societies; these awards play a role in promotions, making them a fundamental building block of success.
Objectives: We aim to explore the gender breakdown among resident awards presented by several Internal Medicine residency programs across the United States in this pilot study. Our ultimate goals are to define disparities in award selection, determine what variables contribute to these disparities, and work to mitigate these variables.
Methods/Research: We generated a survey in REDCap to collect retrospective data about resident award selection from academic Internal Medicine residency programs across the country. This survey gathered awards data from 2009-2019 and included variables such as gender breakdown of the program, gender of resident award recipients, and details about how awards are selected. Eight programs completed the survey; these programs were from six different states in various geographic regions. Overall 43.1 percent of residents were female. Across all residency programs and years, there were 51 distinct resident awards with 290 (39.7%) female winners. Of the 51 distinct awards, there were 10 which were awarded to female residents with the same or higher frequency as males; 6 of these mentioned words that have been differentially associated with women in medicine such as “ambulatory,” “community,” “compassion,” and “humanism.” In the 41 awards favoring males, there was only a single mention of the word “compassion,” and no mention of the others.
Conclusions/Impact: This data shows a concerning disparity in gender of award winners. In the future we will collect data from more residency programs and perform a thorough investigation of selection mechanisms that may help mitigate bias in order to ultimately propose strategies to reduce these gender disparities.
-

Finding a Home: Recognizing the Need for Sex and Gender-Based Medicine Instruction at WMed
A. P. Ho, J. Sassic, and J. Werbinski
Sex- and Gender-Based Medicine (SGBM) is a field that explores the impact of sex as a biological variable and gender as a sociocultural variable on health an illness in all patients. We are arguing that SGBM has been consistently overlooked as an important part of medical education and individualized patient care, contributing to the invisibility of women and gender-nonconforming individuals in medical education, research, and healthcare. Our poster will present the steps taken to introduce SGBM into the curriculum at Western Michigan University Homer Stryker M.D. School of Medicine (WMed) as well as some challenges that WMed and other schools may face in the process. Critical steps include matching SGBM concepts to LCME requirements (“Hot Topics”), faculty and administrative endorsement, and positioning into medical students’ curriculum schedules. A sample lesson plan and recommended resources are outlined as a template to assist other schools in creating or improving upon their own SGBM instructional materials. We also discuss possible ways to improve SGBM curricula, based upon our experiences with the course and methods used to introduce SGBM concepts to additional medical students.
-

The impact of sex and gender in health and disease: an elective
N. Lindsay and T. Rohr-Kirchgraber, MD, FACP, FAMWA
Presentation: 6:12
Historically, “women’s health” has referred to health issues relating strictly to reproduction. The last decade has witnessed an exponential increase in research and understanding of the important role biological sex and gender identity play in health and disease. Sex and gender based differences have been found in nearly every aspect of medicine: most well known among them are differences in cardiovascular and cerebrovascular disease. Much of what we know about pathophysiology and pharmacology is limited by research that has been and continues to be performed mainly in male models. The IU National Center of Excellence in Women’s Health Sex and Gender elective provides an overview of sex and gender specific clinical medicine within a systems-based curriculum. The elective focuses on each body system, where the student explores sex-based differences in epidemiology, pathophysiology, treatment, pharmacology, and outcomes as well as the role gender identity plays as a social determinant of disease. The overarching goal of the rotation is to integrate sex and gender-based evidence into existing curricula, both internal to and external to IUSM. By the end of the elective, the students contribute to the research and development of sex and gender educational tools that can be used to in our current educational programs and beyond. The student also participates in clinical programs with the IUNCOE Women's Wellness on Wheels program, attends clinical sessions in the IUHP Glendale primary care, and attends educational programs throughout the institution to help define best practices that incorporate sex and gender. Completed projects include slide sets created for the Laura Bush Institute for Sex and Gender, written articles on the impact of sex and gender on cardiovascular health, and completed research projects on diversity.
-

Women Authors in Medicine: A Gender Based Study on Authorship Opportunities and its Implications in Promotions in Medicine
K. Lindstrom and T. Rohr-Kirchgraber, MD
Obtaining first authorship in research and published papers is widely held as grounds for promotions and advancements in the medical field. However, the opportunities to be involved in research and to have the primary authorship position are not equally divided amongst specialties, including primary care. Women physicians are becoming a greater percentage of the workforce in primary care, including Internal Medicine and the potential lack of opportunity for authorship may disproportionately affect their promotion. This poster presents the preliminary research on an investigation into the Indiana University School of Medicine’s Department of Medicine gender authorship profiles in the last five years. By utilizing the search engine scopus, a database of the papers written by physicians was created, and gender identifications of the first, second, and last author was made to find correlations between gender and authorship positions. These results will be used to make a case for reexamining the qualifications for promotions, and ensuring that genders have equal opportunity for job advancement and leadership in the medical field.
-

The Evolution of Gender Specific Medicine Education: a historical overview
A. M. Lopez, MD, MPH, MACP
Background: Recognizing the lack of uniform reproductive health education inmedical schools, the American Medical Women’s Association (AMWA) founded theReproductive Health Initiative (RHI) in 1993.
Outcomes: In 1996, the RHI ModelCurriculum was unveiled. In 2004, AMWA presented results indicating that theCurriculum was used in about half of all U.S. medical schools (students/residents)and in 24 countries.
Historical Factors: In 2001, the Institute of Medicine publishedits report, Exploring the Biological Contributions to Human Health: Does SexMatter? arming that “every cell has a sex”! In 2004, the Principles of GenderSpecic Medicine were published and dened gender specic medicine as “how biological sex and the sociocultural aspects of gender aect health and illness for women and men”. In 2005 the Association of Professors of Gynecology and Obstetrics and the National Centers of Excellence in Women’s Health partnered with the Association of American Medical Colleges to align medical schooleducation content and learning objectives. Medical schools began using the modelcurriculum outside of reproductive health education. In 2008, the ndings of asurvey of medical students was released and revealed that students perceived thattopics related to sex and gender dierences had only brief to moderate coverage. Similar results exist across the health professions in nursing, pharmacy, dentistry. In 2015, the NIH announced that sex as a biological variable would be factored intoresearch designs, analyses and reporting.
Current Directions: In 2006, AMWAestablished the Women’s Health Working Group. Building on the work outlinedabove, interprofessional educational eorts were developed based oncompetencies that integrated social determinants, lifespan and culture.
FutureDirections: In 2016, the first Sex and Gender Health Education Summit was hosted by the Mayo Clinic; in 2018, by the University of Utah Health, and in September 2020 by Thomas Jefferson University with an interprofessional focus.
-

AMWA IGNITE: A Novel Program for Medical Students Addressing the Unique Challenges Faced by Women in Medicine
R. E. Melikan, MS, BA; H. L. Shuman, BS; J. A. Files, MD; C. Stonnington, MD; M. Kraus, MD; and J. M. Kling, MD, MPH
Background: Women physicians are more likely than their male counterparts to experience gender discrimination, sexual harassment, role conflict, burn out, and issues related to reproduction. Currently, there is no medical school program that addresses these challenges. AMWA Ignite was developed by female physicians to educate medical students on ways to enhance their careers, navigate the challenges women are more likely to experience, and help mitigate burnout.
Objectives: To develop a curriculum, research opportunities, and coaching for medical students that explores and offers solutions to the unique challenges faced by women physicians in training.
Methods/Research: Two US medical school American Medical Women’s Association (AMWA) chapters participated in the pilot study: Wayne State University in Detroit, Michigan and Mayo Clinic in Scottsdale, Arizona. AMWA Ignite offers three modes of engagement: Curriculum: Expert faculty present topics including reproductive life planning, resilience, sexual harassment, financial wellness, mentorship, intersectionality, and navigating male-dominated specialties.
Topics are determined by the individual chapters with the help of a faculty champion. The modules vary between didactic lectures, case presentations, physician panels, small group discussions, and role playing. Content refinement occurs through pre- and post-session participant surveys. Attendance has been considerable and initial feedback has been positive. Survey results are undergoing analysis and will be available for future presentation.
Research: The modules stimulate ideas for research topics that students can pursue with a faculty advisor. The research component aims to mentor students through the scientific method.
Mentorship: This program has developed one-on-one and group coaching for women, utilizing technology to allow long-distance mentorship.
Conclusions/Impact: AMWA Ignite is an innovative sex and gender specific program that aims to address challenges faced by women physicians. Preliminary data from surveyed medical students has shown interest in this program, which will begin its expansion phase in the academic year 2020-2021.
-

Assessing UCSF Health Trainees' Preparedness to Address LGBTQIA+ Health
B. Morgan, G. Essex, and M. Le
HONORABLE MENTION
Objectives: Lesbian, gay, bisexual, transgender, and queer (LGBTQ) populations face health disparities linked to discrimination and social stigma that can limit access to healthcare. This project expands a 2018 study at UPenn investigating healthcare trainees’ preparedness to treat LGBTQ patients which found that dental students at University of Pennsylvania were signifcantly less interested in receiving formal LGBTQ health education than their peers in medicine. Our survey aims to assess UCSF predoctoral health professions students’ comfort level, attitudes, and preparedness to care for LGBTQIA+ patients in order to investigate how well UCSF is preparing its students to address this community’s health needs.
Methods: Survey questions were adapted from the Greene et al. (2018) study to arrive at a seventeen-item questionnaire. We expanded the scope of the original study from dental, medical, and nursing students to also include students in UCSF pharmacy and physical therapy programs. The new Qualtrics survey was sent to students via UCSF Listservs. Basic demographic information was collected but the survey was otherwise anonymous. 218 responses were compared across program and gender/sexual minority status.
Results:Dentistry, Nursing, and Pharmacy students rated their program’s culture as significantly less welcoming toward members of the LGBTQIA+ community than Medicine and Physical Therapy students (p
Conclusion: Health trainees at UCSF have expressed interest in learning more about LGBTQIA+ health issues, and school curricula should reflect this demand by integrating additional courses/lectures on the topic to increase student readiness and improve patient outcomes.
-

The need for LGBTQ+ education in cancer care: survey results demonstrating provider knowledge gaps about cancer screenings for sexual and gender minority patients
N. G. Nelson, A. P. Smith, Ko K. Kevin, J. F. Lombardo, A. Shimada, A. E. Leader, R. Murphy, and N. L. Simone
BACKGROUND: The National Cancer Institute designates the LGBTQ+ community as medically underserved, leading to differential cancer outcomes. It has been established that LGBTQ+ patients have lower cancer screening rates, which is likely multifactorial, involving emotional distress surrounding medical encounters and gaps in health knowledge. This puts the onus on providers to provide a clinical environment that is culturally competent, well-versed in LGBTQ+ care, and informative for patients.
OBJECTIVES/METHODS: To assess the attitudes and knowledge of cancer care providers regarding health and screening for LGBTQ+ patients, we distributed a 20-item survey to physicians in primary care and oncology subspecialties (n=355).
RESULTS: Providers were more likely to report having formal LGBTQ+-related training if they were female, had less than ten years of practice, or practiced family or internal medicine. These specialists were more likely to agree with the importance of knowing patients’ sexual orientation, despite the fact that every specialty agreed that the LGBTQ+ community experiences different health issues. By specialty, respondents disagreed about which cancer screenings are indicated for certain subpopulations; specialists disagreed whether lesbian women, trans men, and trans women should have mammograms. Responses indicated that some providers were not clear on LGBTQ+ terminology; 36% of providers believed trans women should have pap smears. Seventy-one percent of respondents (and a majority from each demographic) agreed that their clinics would benefit from training about LGBTQ+ health issues. Only 46% of respondents reported confidence in their understanding of health concerns unique to the LGBTQ+ community.
CONCLUSIONS/IMPACT: These responses instantiate the need and desire for LGBTQIA+ education for cancer care providers, including details about health considerations for transgender patients and clearer standards of cancer screening for different subpopulations. From there, providers could deliver better healthcare and patient education to improve the disparity in cancer outcomes noted in the LGBTQ+ community.
-

Revolutionizing Health Care Access: Developing a Mobile App for Women and LGBTQIA+ Community Members
V Newell, BA; D. Jack, PhD, RN; and M. Bouchaud, PhD, MSN, CNS, RN, CRRN
Introduction: People who identify themselves, as members of the LGBTQIA+ community are diverse, coming from all walks of life, and include people of all races and ethnicities, ages, socioeconomic statuses and from all parts of the country. A Meta analysis study conducted by the CDC in 2017 estimates that nearly one million adults in the US is transgender (CDC). Despite the fact that these individuals are members of every community, they continue to experience barriers in accessing health care services such as discrimination, unwelcoming attitudes, and lack of understanding and fear from providers and staff in many health care settings (CDC and GLMA). Consequently, LGBTQIA+ individuals are often reluctant to seek medical care except in situations that feel urgent and even then, many still will not access health care services. Other barriers and challenges that lead to disparity in healthcare for the LGBTQIA+ community mirror those faced by women as well, including lack of reliable and affordable healthcare insurance, high co-pay and hidden fees at the time of payment especially as it relates to sexual healthcare and longer and unexpected wait times. Community resources to inform and guide women and LGBTQIA+ persons of free clinics and healthcare settings that provide culturally competent medical care and prevention services to this population are lacking. This presentation will discuss one authors’ journey to reliable and affordable healthcare as limited and discriminatory and how that led to the development of a survey she designed to understand the user and their thoughts on how to streamline the process of finding a free clinic. The process of developing a mobile geographical application that provides detailed information about community clinics specializing in healthcare services for women and LGBTQIA+ individuals will also be addressed.
Objective: A clear need to provide the community with an application that was easy to use, supply basic logistical information regarding free clinics, and the ability to specify what services were available regarding women’s and LGBTQ+ sexual health.
Methods: Analyzing existing applications that provide similar services presented the shortcomings and successes of what currently exists. Using data from surveys and interviews, user personas helped develop an empathetic understanding of the targeted demographics’ goals, wants, and needs when using the application. Data from a virtual card sort was collected to dictate how the information within the application was arranged. Usability testing with a prototype determined the viability of the design and its effciency in meeting the user's goals.
Results: From participant responses, it was determined that this technology would have tremendous benefits to the under-represented community of women and LGBTQIA+ members seeking qualified, cost prohibitive health care services. Themes gathered from the focus group participants include: • Autonomy • Privacy • Advocacy
Conclusion: Although there is an identified need for this particular mobile application, the prototype remains in a hiatus status as other design assignments have prioritized and occupied the time that could be devoted to this product launch. The intent is to continue to develop this product and make it available in the near future.
-

A Lesson from COVID-19 in the Importance of Sex Disaggregated Data: Sex Differences in SARS-CoV-2 Infection and Mortality Rates
C. Newman, MD, FACP, FAHA, FAMWA and A. Baum, BS
Background: Emerging surveillance data from the COVID 19 pandemic suggest better outcomes in women.
Objective: This analysis aims to determine the magnitude of sex differences in SARS-CoV-2 infection rates and survival at a country level.
Methods: Data was sourced from the Global Health 50/50 (GH 50/50) website https://globalhealth5050.org/covid19, housed at University College of London, which collects government reported national surveillance data on confirmed cases of COVID 19 and confirmed deaths. This analysis used data completely disaggregated by sex, cutoff date 5/8/2020.
Results: Of 78 countries, with 3,044,513 confirmed cases of COVID 19 and 181,742 deaths, data were completely disaggregated by sex in 36 countries, partially disaggregated in 26, and not disaggregated in 16. In countries, with completely disaggregated data, 1,240, 803 cases of COVID-19 were reported on May 3, 4, 5 or 6, 2020 in 31 countries, and between Feb 28 and April 28 in 5 countries. The average proportion of cases in women was 50.3%: range 22% (Pakistan) to 63% (Netherlands). Deaths were reported in 83,388 individuals. The mean proportion of deaths in women was 39.2% (range 20% to 53%). The mean ratio of deaths (men to women) was 1.62 (range 0.9 to 3.2).
Discussion: This analysis of surveillance data from 36 countries shows a sex difference in mortality from COVID-19, with men more likely to die than women. Possible explanations include sex differences in the immune system, gender differences in environmental exposures or access to healthcare, and differences in comorbidities. Additional research to assess potential causes, and collect and analyze data by age, race, and ethnicity as well as sex and gender would be of value. These observations highlight the importance of disaggregating data by sex and gender in order to understand disease susceptibility, prevalence, and outcomes.
-

Diversity of Dermatology Trainees, 2014-2018
S. Oska, B. Partiali, and A. Folbe
Background: Although the U.S. population is becoming increasingly diverse, gender and racial diversity in medicine is lacking. Improving the diversity of the physician workforce can have an important impact on improving health care access and outcomes for underserved patients.
Objective: The objective of this study is to examine trends in sex, racial, and ethnic diversity of trainees in the field of dermatology.
Methods: Graduate medical education supplements published annually in the Journal of the American Medical Association were used to obtain demographic data of dermatology trainees from 2014-2018.
Research: Over the past five years, women have made up the majority of trainees in dermatology. The representation of female residents has remained relatively stable from 2014-2018, with most current data indicating women comprise 60.78% of dermatology residents. When examining resident physicians in all specialty programs, women comprise 45.56% of trainees. Although women have consistently made up the majority of dermatology trainees from 2014-2018, they remain relatively underrepresented in dermatopathology, micrographic surgery, and dermatologic oncology. Over the past 5 years, women have made up 52.80% of trainees in dermatopathology fellowships. Similarly, women have comprised 47.78% of trainees in micrographic surgery and dermatologic oncology.
Conclusions: Dermatology is one of few medical specialties in which women comprise the majority of trainees and a significant portion of the active workforce. Further efforts and initiatives to improve diversity in dermatology residency and fellowship programs may be necessary, especially at the medical student level.
-

Students Take Lead to Educate Faculty on the Use of Sex and Gender Terminology in Pre-clinical Courses
S. Pfister; H. Tolo, M3; R. L. Conger, M4; V. Magana, M3; J. R. Smoko, M3; S. K. La Bodda PHARMD; and S. E. Polhemus
TOP WINNER
Student leaders in the Lesbian, Gay, Bisexual and Transgender People in Medicine student run organization at the Medical College of Wisconsin noticed that curricular language around sex and gender was absent and/or incorrect in the pre-clinical medical school (M1/M2) courses. After reaching out to the M2 Endocrine/Repro Unit course director, students prepared a report to present to all M1/M2 Course Directors.
Objectives: One goal of the report was to “educate the educators” so that faculty would have better understanding of the distinction between sex and gender. Ultimately this would translate to the students and improve overall future patient care.
Methods: A presentation was developed and given at the quarterly M1/M2 course director meeting (Fall 2019). Information included statistics from the 2015 US Transgender Survey which underscored that ignorance surrounding sex versus gender terminology could result in an environment in which patients do not seek care. The student presentation comprehensively explained the definitions of sex, gender, cisgender and transgender. Course directors were given action items to evaluate their courses and afirm that terms were used appropriately. Student leaders provided contact information for faculty feedback.
Conclusions/Impact: In February 2020, students reported of changes in some courses. For example, the M2 cardiovascular unit led off the session on women and heart disease with sex and gender definitions provided by students. Cardiovascular risks of hormonal therapy for transgender patients was included. Students noted that language around sex and gender in the M2 endocrine-repro unit was consistently correct (female not woman when discussing XX fetus). A M1 pharmacology lecture included the student's definition slide as prelude to discussion of male/female differences in drug response. With little effort, students played an integral role in improving curricular content related to sex and gender medicine and further supporting the model that students are important drivers of change.
-

Getting Sexual and Gender Minority Health "Into the Brick and Mortar": A Mixed Methods Implementation Study
M. L. Pratt-Chapman
What predicts medical student knowlege, attitudes, beliefs and behaviors about LGBTQ+ patient care? What lessons have been learned about implementing LGBTQ+ health curricular change?
Students with LGBTQ+ friends or family were 7% more likely to have relevant LGBTQ+ knowledge and 12% more likely to have affirming beliefs about LGBTQ+ patients than students who did not.
More training hours focused on LGBTQI+ health led to more clinically prepared medical students who were more likely to exhibit affirming clinical behaviors for LGBTQ patients. LGBTQ-specific training explained about 15% of the difference between people who felt prepared and those who did not.
-

Prioritizing lesbian, gay, bisexual and transgender health content in a family nurse practitioner program
S. Rainer, PhD, APRN, FNP-BC, ANP-BC, ENP-C; D. Frederick, DNP, FNP-C, CNOR, RNAFA; L. Peoples, DNP, CRNP; and J. Shiro, PhD, RN, APN, FNP-BC
Background: The Family-Individual across the Lifespan (FIAL) program at Thomas Jefferson University College of Nursing implemented significant curricular changes after a formative evaluation of teaching and learning strategies around sex and gender health education. We found a glaring lack of curricular activities geared towards the health needs of the lesbian, gay, bisexual, and transgender (LGBT) community. The curricular changes were implemented to specifically address pervasive health disparities and barriers to high-quality primary health care among LGBT people.
Objectives: 1) Identify barriers and afirm LGBT patients’ unique primary health care needs. 2) Promote Family NP competence in providing care to LGBT people across the lifespan. 3) Develop core competencies that form the basis of best practices for Family NPs caring for the LGBT community.
Methods: The Family NP Faculty designed three (3) Sex and Gender learning modules in the program’s clinical courses. These modules specifically address unique socio-cultural needs, sensitivities, and challenges related to sustained gender-inclusive and gender-afirming care. The first student cohort that completed the Sex and Gender Health Care curriculum completed an anonymous feedback survey.
Conclusions/Impacts: The Family NP program has taken an initial step in providing Sex and Gender Health Education (SGHE) across the curriculum after identifying a need to prioritize lesbian, gay, bisexual, and transgender-specific content. However, based on student feedback from this first step we are revising the modules and providing more opportunities for students to work directly with the community. We are reaching out to community partners to access members willing to share their stories about their health care experience to better inform guidelines and the development of best practices. Many of our students identify as gay, lesbian, and gendernonconforming and provided validation that the Family NP program needs to continue to develop robust Sex and Gender Health Care learning opportunities.
-

Sex and Gender Topics in Medical Student Learners: Follow up
A. M. Rydberg, V. M. Miller, M. Buras, J. K. Quillen, and J. M. Kling
TOP WINNER
Background: In an era of patient-centered, individualized medicine, it is important to consider of the impact of sex and gender on mechanisms of health and disease. Objectives: This study aimed to assess medical students’ current knowledge of sex and gender-based medical concepts and to compare responses to the prior assessment at Mayo Clinic in order to better inform ongoing efforts to improve medical education curricular materials.
Methods: An electronic survey that assessed current knowledge of sex and genderbased medicine was sent to all 1st – 4th year medical students at the Mayo Clinic Minnesota and Arizona campuses. Descriptive and qualitative thematic results were compared to the same survey administered in 2012 to assess the efficacy of curriculum changes in better covering sex and gender-based medicine topics.
Results: A total of 100 of 365 (27% response rate) of students responded, with 2:1 female to male with representation from all 4 years. The terms sex and gender were correctly identified by most respondents (93%). Various medical knowledge questions were answered incorrectly. Students reported many areas where concepts of sex and gender were not routinely covered n including orthopedics and nephrology, although these percentages have increased since 2012. Sixty two percent of students favored increasing sex and gender health concepts in the current curriculum.
Conclusions: Medical students appear to understand the definition of and importance of sex and gender. While some improvements in coverage by topic area have occurred, opportunity remains to more fully integrate these concepts in medical school curricula.
-

Decreasing the threat to learning: the impact of gender ratio in clinical skills small groups
A. Schoenberger, BA, MSEd; H. Christensen, PhD; and S. Overlam MS
Background & Objective: Small-group learning is a popular fundamental teaching strategy in undergraduate medical education (UME). Evidence of women acting as “social vaccines” for their women peers in small groups has been described in engineering, but not in UME. We seek to better understand the impact of smallgroup gender composition on medical student learning.
Methods: Preclinical medical students were surveyed throughout their clinical skills (CS) course. Likert-scale questions measured students’ perception of their simulation encounters as challenging or threatening, and data were used to calculate a challenge-to-threat ratio (CTR). Scores >1 indicated a situation more challenging than threatening, whilesurvey.
Results: Survey response rates ranged from 62.6-78.8%. Average CTRs of firstyear students were higher for men (1.52-1.64, n=62) than women (1.23-1.46, n=71). All CTRs decreased at the start of the second year (0.80-1.40, n=108), but rebounded as student training progressed (1.29-2.36, n=118). Early second-year CS group gender composition did not impact men (similar CTRs ranging 0.83-1.09). However, women reported a disparate CTR across groups with one, two, and three women (0.80, 1.40, and 1.38 , respectively). Late second-year students reported the highest CTRs in groups with gender parity and lowest CTRs in groups with only one female student. Sentiment analysis of open comments shows a gender effect, with more negative sentiments from women.
Conclusions: Women were less confident than their male peers in the early CS small-group learning environment. Less confidence for all students was reported as CS cases progressed in the second-year to an internal medicine focus; however, confidence recovered in the late second year. A significant threat was perceived by the sole woman in a small group, but the presence of 1-2 other women appeared to be protective against this effect on confidence.
-

Chronic pain: the importance of a sex and gender-based approach to treatment
A. Sedaghat and T. Rohr-Kirchgraber
Twenty-eight million women in the United States suffer from chronic pain. 70% of patients seeking treatment for chronic pain are women, and are found to return to pain clinics thirty-two times more frequently than men. These findings indicate that women experience insuficient pain relief following intervention. Given that 80% of pain research has been conducted on men, most knowledge of pain pathways in women are extrapolations, shedding light on the ineficiencies of current treatment algorithms, and the importance of a sex and gender-based approach to chronic pain.
The biochemistry and physiology of the pain pathway, as well as the pharmacokinetics and pharmacodynamics of medications used to remedy pain responses, are signifcantly different between men and women. Low-estradiol states result in a reduction in both mu-opioid receptor recruitment and basal activation, leading to significant hyperalgesia and sensitivity to chronic pain in women as compared to men. Further compounding the dichotomy between the chronic pain response is the response to analgesics. Women have lower levels of glucuronidation, higher volumes of distribution, and lower clearance of commonly administered analgesics as compared to men. Psychosocial factors such as gender roles, expectations surrounding pain, and coping strategies also determine how pain is perceived and ultimately influence how pain is treated. These findings are just beginning to shed light on the ways in which women and men respond differently in vivo to pain. However, the decision to treat women and men as separate entities with respect to pain management should not be a binary one. While patients should be treated as individuals, pre-menopausal, post-menopausal and transgender women, should all be met with an approach that takes into account the sex and gender differences that exist. Pain management physicians should take heed of these complex differences and utilize a sex and gender-based approach while managing patients.
-

One Institution’s Multidisciplinary Approach to Integrating Education of Gender Minority Health into Medical Curricula
M. Snyder, A. Sevem, G. Enciso, A. Stage, L. Wellman, B. Hooper, N. Sriraman, and M. Kannarkat
Background: Compared to the general population, transgender and gender diverse (TGD) individuals have poorer health outcomes and experience greater healthcare barriers. Current literature describes these inequities as directly related to a lack of provider knowledge and inexperience interacting with TGD people. A preliminary review of our institution’s preclinical curriculum demonstrated content geared mostly toward modifying attitudes via reflective exercises and patient panels. In order to increase the breadth of our curriculum, we developed a multidimensional approach that specifically assesses and enhances provider knowledge, and offers clinical opportunities for learners to meaningfully engage with TGD individuals.
Objectives: To develop a curriculum that trains future physicians to provide gender affrming, patient-centered care for TGD patients.
Methods: To assess for and characterize gaps in TGD curriculum among medical students, we surveyed our institution’s curriculum using a key-word driven map, the findings of which are informing conversation and inspiring necessary reform. To enhance TGD knowledge among residents, we are working alongside the Pediatrics and OB/GYN residency programs to develop a standardized curriculum that offers field-specific training on navigating conversations regarding sex and gender. The efficacy of these training sessions will be evaluated using pre- and post-survey responses, which will inform future training sessions. To increase exposure and opportunities to provide care for TGD patients along the continuum of medical education, we expanded services at our student-run free clinic, developed a clinical elective, and are integrating experiences into the OB/GYN core clerkship.
Impact: Here, we lay the framework for how one institution is characterizing gaps in education and integrating TGD health topics longitudinally across undergraduate and graduate medical education curricula. This work has the potential to impact curriculum development initiatives at other institutions seeking to better prepare their learners to care for TGD patients.
-

Using a Hybrid Lecture and Small Group Standardized Patient Case to Teach the Inclusive Sexual History and Transgender Patient Care
S. Stumbar, N. A. Garba, M. Stevens, E. Uchiyama, E. Gray, and P Bhoite
Background: Previous negative experiences with the medical community often leave transgender people reluctant to seek needed medical treatment and preventive care. Inadequate training in transgender healthcare during all stages of medical education promotes the disparities experienced by this community. Undergraduate medical education is uniquely positioned to address these disparities by better preparing future physicians to provide inclusive care to transgender patients; however, curricular coverage of these topics remains inadequate.
Methods: The second-year clinical skills course at the Herbert Wertheim College of Medicine includes a hybrid workshop consisting of a one-hour lecture about the components of an inclusive sexual history, followed by a 1.5 hour, faculty-facilitated small group session during which students interview a standardized patient playing the role of a transgender man with abdominal pain. During the session, students were provided with an optional, anonymous pre- and post-intervention survey assessing the impact of this workshop.
Results: After the session, there was a statistically significant increase in students’ knowledge of the Create your own automated PDFs with JotForm PDF Editor 1 components of an inclusive sexual history, in the number of students who felt that their medical training had effectively prepared them to provide medical care for transgender patients, and in those who reported feeling comfortable gathering a sexual history from a transgender patient. Students overall reported a high level of satisfaction with the session and the standardized patient case.
Conclusions: Our findings suggest that the hybrid-learning format of the sexual history workshop effectively improved students’ knowledge and confidence regarding transgender healthcare and sexual history taking. Although our case was acted by well-coached cis-gender standardized patients without the lived experiences of being transgender, students still reported that it provided a realistic opportunity to explore the nuances of transgender healthcare. While we demonstrated value in using cis-gender standardized patients, future directions of this project will explore the recruitment of transgender standardized patients.
-

Reporting of Sex Specific Outcomes in High Impact Orthopedic Journals
K. Stumpff, MD; M. R. Hadley, MD; and K. J. Templeton
Background: There are known biologic differences between men and women that affect all aspects of health and disease, including in orthopedics. Hormonal regulation influences bone density, tissue structure, joint laxity, and muscle mass. Differences in anatomy and neuromuscular control have also been identified. While previous studies on disease incidences have shown certain conditions are more common in one sex (e.g., osteoarthritis in women), it is not routine practice to evaluate or publish outcomes based on sex.
Objectives: To evaluate the frequency with which papers in orthopedic journals published sex-specific outcomes with regard to knee osteoarthritis and rotator cuff pathology.
Methods: Four high-impact orthopedic journals were reviewed: Journal of Bone and Joint Surgery (JBJS), Clinical Orthopedics and Related Research (CORR), American Journal of Sports Medicine (AJSM), and Journal of Arthroplasty (JOA). JBJS and CORR were reviewed for rotator cuff and knee osteoarthritis. AJSM was reviewed for rotator cuff, while JOA was reviewed for knee osteoarthritis. 100 articles from each journal were reviewed. If there was any further analysis of sex beyond the statement of how many men and women were included in each group, a study was designated as successfully reporting sexspecific outcomes.
Results: 24-29% of rotator cuff articles reported on sex-specific outcomes. Sex specific outcomes were reported in 32-40% of knee osteoarthritis publications. Comparing rotator cuff to knee osteoarthritis articles, there was a trend toward more publications with sex-specific outcomes in knee osteoarthritis, however, this was not statistically significant (p = 0.0562). JBJS publishes significantly more articles reporting sex specific outcomes regarding knee osteoarthritis than rotator cuff (p= 0.0156).
Conclusions: Sex-specific outcomes are not widely reported in high-impact orthopedic journals. Sexspecific outcomes are reported more often in knee osteoarthritis where there are already well-known sexbased differences. To improve care, sex-specific outcomes should be reported across all orthopedic conditions.
-
 by B. A. Sweeney, A. Carcieri, A. M. Falleni, L. A. Gatewood, M. L. Rodriguez, H. Bell, A. Croke, and P. G. Clark")
Innovative Interprofessional Collaboration: Addressing the Need for Education for Health Center Workers around Patients' Sexual Orientation and Gender Identity (SOGI)
B. A. Sweeney, A. Carcieri, A. M. Falleni, L. A. Gatewood, M. L. Rodriguez, H. Bell, A. Croke, and P. G. Clark
BACKGROUND: University of Rhode Island (URI) students in a graduate-level course, Interdisciplinary Teamwork in Health and Human Services, collaborated with a local health provider, Wood River Health Services (WRHS), to create training materials for its staff on the topic of sexual orientation/gender identity (SOGI). WRHS is a federally-funded, comprehensive community health center located in a rural area of Rhode Island. It provides medical, dental, and mental health services. WRHS had been advised to enhance its attention to issues related to SOGI.
OBJECTIVES The aims for this project were: 1. Assess needs and priorities of WRHS staff around knowledge and attitudes about SOGI and health care; 2. Create a training tool for staf fto enable them to facilitate patient comfort in disclosing SOGI-related information that would assist them in addressing individual needs of patients; 3. Provide students an opportunity to effectively learn and practice interprofessionally.
METHODS The students--representing three different health fields (Occupational Therapy, Human Development and Family Studies, and Pharmacy)--researched SOGI issues related to their fields. Students met with WRHS staff to develop a clear understanding of the center’s barriers to adequately provide care to LGBTQ+ patients. They conducted a survey to assess staff attitudes and knowledge about SOGI terminology, health disparities, and the importance of a welcoming environment that informed the development of a training presentation. Staf can complete it at their convenience, and it can be used as part of onboarding new staff. Retrospective pre/post-tests were administered to students and WRHS staff.
CONCLUSION Informational presentations are a useful tool for agencies looking to build capacity and comfort among staff around SOGI. Additionally, providing students with opportunities to learn with, from, and about each other is a critical component of health professions education.
-

Outpatient Primary Care Practitioner Access: Sex-Based Preferences
G. Taylor, K. Poole, M. Girardo, and J. Kling
Background: In some innovative outpatient practice models, patients are faced with trade-offs, such as choosing between continuity of care vs quick access to a healthcare practitioner (HCP). Our objective was to assess sex-based differences in visit access preferences at an academic outpatient internal medicine clinic.
Methods: A 13-question survey with four discrete choice experiments proposing hypothetical care scenarios was offered to patients over a 6-week period in 2018. Descriptive statistics and chi-squared tests evaluated results by sex for categorical variables, Mann-Whitney rank-sum test for continuous variables, and multivariable models adjusted for age, marital status, education, and income. P-values < 0.05 were statistically significant.
Results: A majority of 796 of 1731 (46%) respondents were female (56%) and over age 65 (58.5%). Females were more likely than males to prefer communicating with the same allied health staff (AHS) over receiving a quick response (female 36.3% vs male 28.0%, p=0.0031) Females prioritized seeing their own provider as opposed to scheduling a convenient appointment for routine care (female 90.2% vs male 85.0%, p =0.028). Multivariable analysis found that females were 6% less likely than males to request the same AHS for communication (95% CI 0.62-1.44), 29% less likely to request the same HCP for yearly physicals (95% CI 0.34 – 1.44), but 3% more likely than men to request an acute visit with the same HCP (95% CI 0.68-1.56) and 13% more likely to request the same HCP for virtual visits (95% CI 0.70-1.81).
Conclusion: Sex-based differences in access preferences were identified. Women preferred continuity of care with the same HCP and AHS over ease of scheduling or a quick response, though these preferences appear to be moderated by other factors including age and marital status. Further identification of longitudinal and socioeconomic factors influencing preferences is needed in this era of evolving practice models.
-

"Sex and Gender-Based Women's Health: A Practical Guide for Primary Care" - A Resource for Learning and Teaching
S. Tilstra, B. M. Dolan, J. L. Mitchell, M. P. Carson, and D. S. Kwolek
TOP WINNER
Background: Patients expect comprehensive, gender-specific care; yet studies reveal that few residency programs in internal medicine provide dedicated training in women’s health and gender-based medicine. Further, graduates are unable to demonstrate competency to care for female and gender-diverse patients.
Objectives: To produce a sex and gender-based women’s health curriculum, written explicitly for primary care providers to guide the care of women and gender-diverse patients, and to be used as a curriculum to educate learners.
Methods: In collaboration with Springer Nature, development of this online and inprint textbook began in 2017. Topics were chosen with input from women’s health experts and are tailored to gender-based conditions commonly evaluated, diagnosed, and/or managed in the primary care setting. Authors were then recruited nationally for each topic. Using evidenced-based medicine principles, chapters were formatted for consistency to include the epidemiology, physiology/pathophysiology, clinical manifestations, differential diagnosis, diagnostic approach, and treatment for each topic, when appropriate. Each chapter has clear, measurable learning objectives, summary statements, and multiplechoice questions with annotated answers to check understanding and help earn CME and MOC credit. With 39 chapters and >600 pages, sections are comprehensive and include Breast and Gynecologic Health and Disease, Obstetric Medicine, Chronic Pain Disorders, Mental Health and Trauma, LGBTQ Health, Common Medical Conditions (osteoporosis, cardiovascular disease), and Foundations of Women’s Health, which highlights the history, disparities, and future of women’s and gender-based healthcare.
Conclusions/Impact: This is the first comprehensive curricular resource written by clinical women’s health physicians, using the most up-to-date evidence, clinical guidelines, expert opinion, and clinical pearls. Our goal is to provide a guide that can serve as a quick point-of-care clinical reference for a specific topic or as a longitudinal curriculum for learners in any primary care discipline, especially programs where women’s health and gender-specific curricula and champions are sparse.
-

Undergraduate Medical Education Sex- and Gender-based Education: An Institutional Audit and Integration Project
H. Turnerm MD; E. Snyder, MD; A. Das, MD; R. Godby, MD; M. Guthrie, MD; S. Kumar, MD; and L. Walter, MD
Background: While evidence-based medicine (EBM) supports the incorporation of Sex- and Gender-based Medicine (SGBM) into patient care, a significant gap exists in its translation to current undergraduate medical education (UME). Several studies assessing medical student and resident physician knowledge regarding SGBM demonstrate suboptimal awareness, knowledge base, and clinical incorporation. There is urgent need to evaluate UME under a SGBM-focused lens, to emphasize the existing SGBM content, and to identify additional opportunities for inclusion.
Method: Lectures from two pre-clinical UME modules, ‘Cardiovascular’ (CV) and ‘Musculoskeletal/ Dermatology’ (MSK/Derm), at the University of Alabama at Birmingham School of Medicine were subjected to a SGBM taskforce audit. Taskforce auditors were tasked with 1) assessing for pre-existing inclusion of SGBM as well as 2) opportunities for SGBM incorporation. Opportunities for inclusion were identified by a taskforce SGBM expert. Evidence-based SGBM material (e.g. slides) to fill the opportune gaps were subsequently created for module director consideration and ready incorporation. Post-audit follow-up of SGBM incorporation and uptake was completed for both modules.
Results: Sixty-four lectures in the MSK/Derm and 23 CV lectures were reviewed by the SGBM audit taskforce. Approximately a third (36%) of all sessions included an element of pre-existing SGBM material (35% of CV; 36% MSK/Derm). Fourteen CV-specific SGBM opportunities were identified, and correlative SGBM inclusive material, was given to the CV module directors; thirteen of these were incorporated (92.8%). Nine MSK/Derm-specific SGBM opportunities were identified with correlative SGBM-inclusive material provided; two (22%) of these were incorporated.
Conclusion: Inclusion of SGBM into medical school curriculum is important for comprehensive medical education and ultimately, for patient care. Identifying and collaborating on SGBM educational opportunities will be crucial for its timely uptake into the UME world. The creation of a dedicated taskforce which searches for inclusion opportunities across the curriculum is one approach to increase SGBM within UME.
-

The Role of Gender in Nurse-Resident Interactions: A mixed-methods study
N. Zanielm, MSc2; E. C. Manchanda, MD, MPH1; A. N. Chary, MD; L Nadeau, RN3; J Verstreken, MSN, MBA/MHCA RN4; E. Shappell, MD3; W. M. Konstantopoulos, MD, MPH3; and V. Dobiesz, MD4
Background: Gender disparities continue to persist within the medical field. Adverse effects of gender bias are well documented, including among trainees in Emergency Medicine (EM). The extent to which gender bias affects interprofessional interactions is not well understood.
Objectives: The study aimed to understand perceptions and experiences of gender bias in interactions between emergency medicine (EM) residents and emergency department (ED) nurses.
Methods: This mixed-methods study involved eight key informant interviews and two focus groups, and an anonymous electronic survey administered to EM residents and nurses at two teaching hospitals. Quantitative analysis included descriptive statistics and between-group comparisons using Student t-tests and two-sample Wilcoxon rank-sum. Qualitative analysis used a inductive and thematic content analysis.
Results: Most participants identified gender as an important factor in ED interprofessional relationships. Key themes emerging from qualitative data include differential treatment and communication styles based on gender. 134 individuals completed the survey: 104 nurses (29% response rate), 30 residents (53% response rate). Females more frequently reported experiencing interprofessional gender bias than males [mean 30.9 (95% CI 25.6-36.2) vs 17.6 (95%CI 10.3-24.9)]. Residents of both genders reported witnessing interprofessional gender bias more frequently than nurses [mean 58.7 (95%CI 48.6-68.7) vs 23.9 (95%CI 19.4-28.4)]. Residents, compared to nurses, more frequently felt gender bias affects job satisfaction (p=0.002) and patient care (p=0.001). These differences were largely driven by female residents’ responses.
Conclusion/impact: Gender plays a significant role in shaping interprofessional interactions in the ED. Gender bias in interprofessional interactions contributes to workplace dissatisfaction, particularly for female residents. Initiatives to establish equitable relationships across the gender spectrum in EM are needed to address interprofessional gender bias.
-

Faculty Development As a Tool to Impact Culturally Competent Care of Sexual and Gender Minorities
A. Zapletal, OTD, OTR/L, CLA; T. Vause-Earland, PhD, OTR/L; S. Toth-Cohen, PhD, OTR/L; and K. A. Bell, PT, DPT, GCS
Presentation: 5:39
Background: This poster focuses on the integration of faculty development of sexual and gender identity health knowledge and skill into health education. There is a gap in inclusion of this content in health professional curriculum. While awareness of LGBTQ+ population health has been indirectly addressed within curriculum, a consistent approach targeting all coursework and faculty can increase culturally competent care of patients that identify as LGBTQ+. Faculty confidence, awareness, and experience regarding knowledge, respectful terminology, and skill directly impacts the likelihood of students becoming culturally competent practitioners.
Objectives: The objectives of this poster are to share outcomes of faculty development. This poster will: ● Discuss integration of faculty roles in academia and health profession accreditation standards with theories of cultural competence and humility inclusive of sexual and gender minorities; ● Describe a faculty development program to build foundational understanding of respectful terminology to optimize trust and respect when conversing with/about individuals within sexual and gender minority populations; ● Demonstrate changes in knowledge, awareness, skill, and perceived comfort with sexual and gender minority communities following participation in the program.
Methods/ Research: Monthly structured learning sessions were paired with 20-30 minute mentoring check-ins with Sexual and Gender Minorities Education and Training (SG-MET) faculty to address components of LGBTQ+ inclusive curriculum. Pre, mid, and post surveys, composed of open and close-ended questions, assessed satisfaction and changes in knowledge, awareness, and perception of skills. Standardized assessments of sexual and gender minority knowledge, experience and clinical skills were completed and collected anonymously through an electronic survey system to protect the faculty’s identification.
Conclusions/ Impact: This faculty development program provides pilot data to suggest that this is an effective way to increase knowledge, awareness, and skills in the area of sexual and gender minority health content delivery and practice to impact healthcare disparities in these populations.

{kind=link}
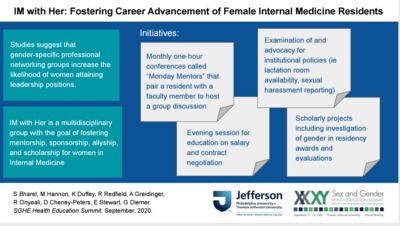{kind=link}
{kind=link}
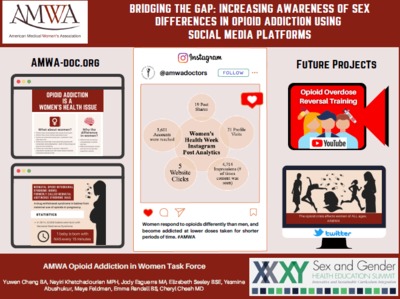{kind=link}
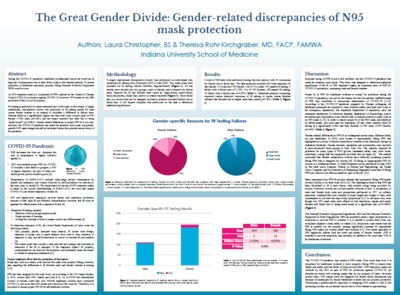{kind=link}
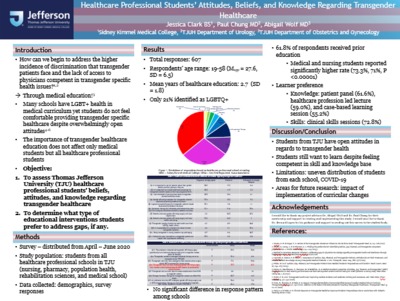{kind=link}
{kind=link}
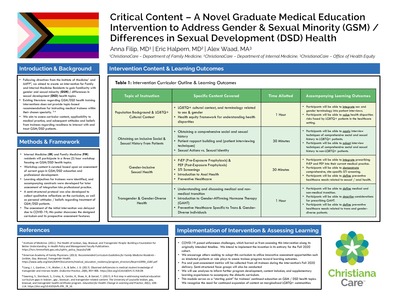{kind=link}
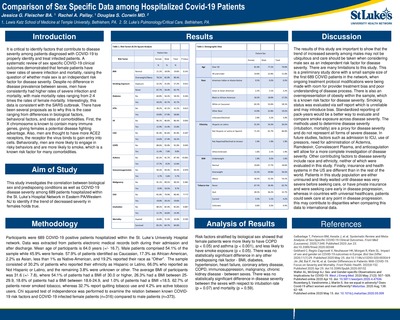{kind=link}
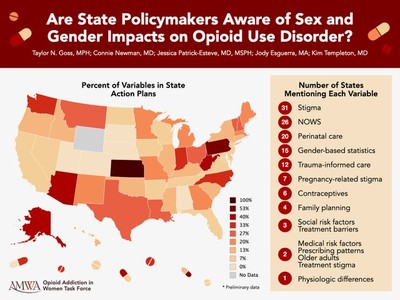{kind=link}
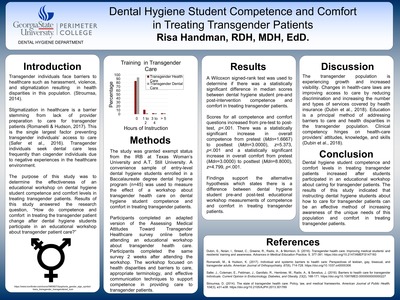{kind=link}
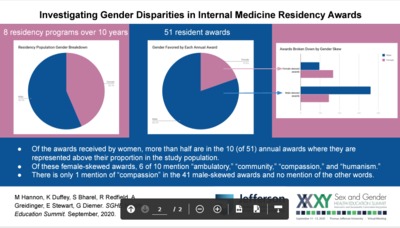{kind=link}
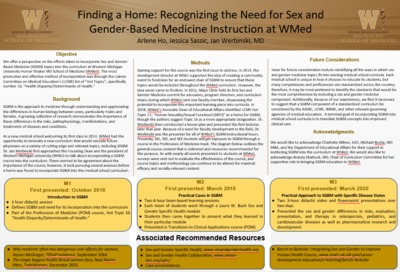{kind=link}
{kind=link}
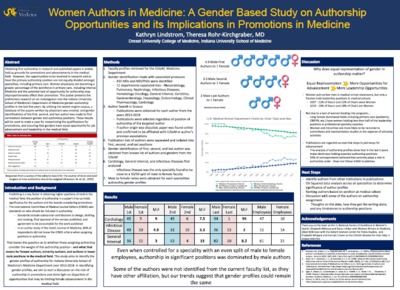{kind=link}
{kind=link}
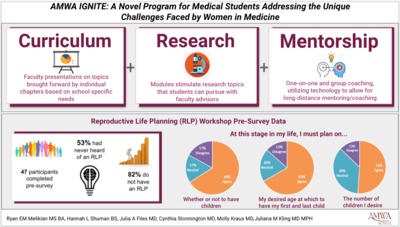{kind=link}
{kind=link}
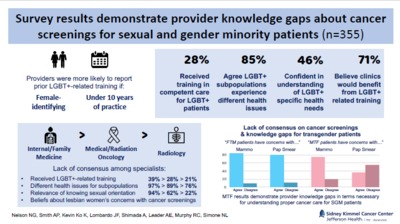{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
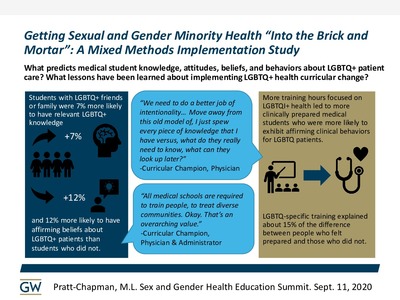{kind=link}
{kind=link}
{kind=link}
{kind=link}
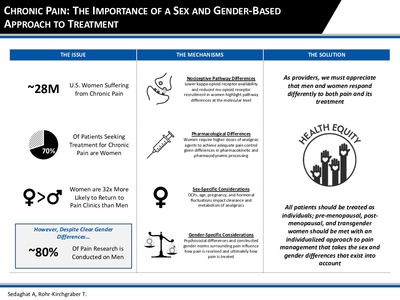{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
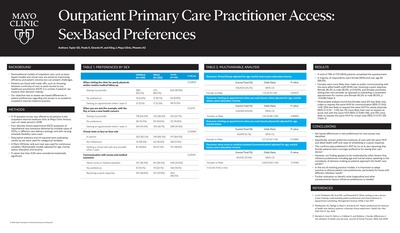{kind=link}
{kind=link}
{kind=link}
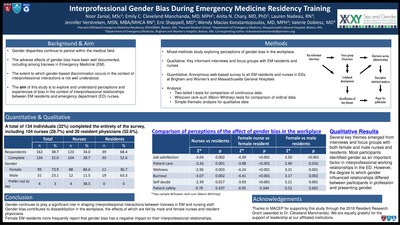{kind=link}
{kind=link}