

-

Comparing Treatment Effectiveness and Patient-Reported Outcome Measures of Four Treatment Options for Obstructive Sleep Apnea
Robert Diecidue, DMD, MD, PhD, MBA, MSPH; Joseph Harrington, BS; Erika L. Manning, PhD, MD, MPH; and Colin T. Huntley, MD
Abstract
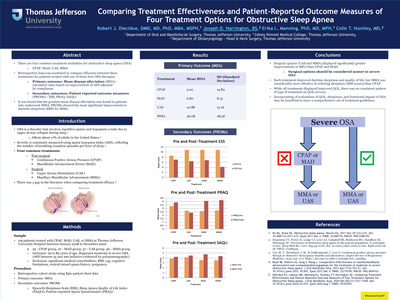
- There are four common treatment modalities for obstructive sleep apnea (OSA)
- CPAP, MAD, UAS, MMA
- Retrospective data was examined to compare efficacies between these treatments for patients treated with one of these four OSA therapies.
- Primary outcome: Mean disease alleviation (MDA) - calculated value based on improvement of AHI adjusted by compliance.
- Secondary outcomes: Patient reported outcome measures (PROMs) - ESS, PRAQ, SAQLI
- It was found that the greatest mean disease alleviation was found in patients who underwent MMA. PROMs showed the most significant improvement in daytime sleepiness (ESS) for MMA.
-

Intraoperative Evaluation of Nasal Valve Repair Interventions: A Prospective Analysis
Kurren Gill, MD; S. Hamad Sagheer, BS; Cory Bovenzi, MD; Brian Yan, BA; Howard Krein, MD, PhD; and Ryan Heffelfinger, MD
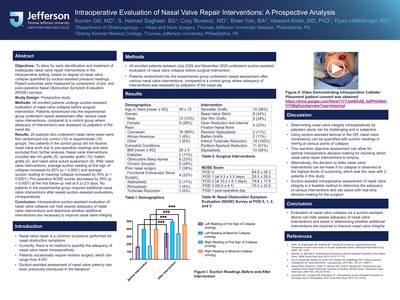
Objectives: To allow for early identification and treatment of inadequate nasal valve repair interventions in the intraoperative setting, based on degree of nasal valve collapse quantified by suction-assisted pressure readings. Patient outcomes were measured by comparison of pre- and post-operative Nasal Obstruction Symptom Evaluation (NOSE) surveys.
Study Design: Prospective study.
Methods: All enrolled patients undergo suction-assisted evaluation of nasal valve collapse before surgical intervention. Patients randomized into the experimental group underwent repeat assessment after various nasal valve interventions, compared to a control group where adequacy of interventions was assessed by palpation of the nasal ala.
Results: 20 patients who underwent nasal valve repair were first randomized into control (10) or experimental (10) groups. Two patients in the control group did not receive nasal valve work due to pre-operative readings and were excluded from further analysis. Nasal valve interventions included alar rim grafts (5), spreader grafts (10), batten grafts (2), and nasal valve suture suspension (8). After nasal valve interventions, average suction reading at first sign of collapse increased by 92% (p < 0.0001) and average suction reading at maximal collapse increased by 16% (p < 0.0001). Pre-operative NOSE scores decreased by 55% (p < 0.0001) at the first follow-up visit at 9.3±3.5 days. No patients in the experimental group required additional nasal valve interventions after repeat suction-assisted evaluations intraoperatively.
Conclusion: Intraoperative suction-assisted evaluation of nasal valve collapse can help assess adequacy of nasal valve interventions and determine whether additional interventions are necessary to improve nasal valve integrity.
-

Fat Graft for Parotidectomy Defect Reconstruction in the Setting of Malignant Disease
S. Hamad Sagheer, BS; Alexander Knops, BA; Kurren Gill, MD; Vivian Xu, BS; Howard Krein, MD, PhD; and Ryan Heffelfinger, MD
Objectives: Currently, limited data examines the safety of utilizing fat transfers in the setting of malignant parotid disease. Here we evaluate the safety of fat graft reconstruction of parotidectomy defects in the setting of malignant disease.
Study Design: Retrospective cohort study
Methods: Electronic chart review of patients who underwent parotidectomy from 2012-2020 were reviewed.
Results: Three hundred and sixty-one patients were identified at a single institution who underwent parotidectomy, and 113 (31.3%) were for malignancy. One hundred and thirty-two patients underwent fat graft reconstruction (49.2%, n=65 for umbilical, 50.8%, n=67 for dermal). One-third of patients had malignant pathology (34.8%, n=46). The most common malignant tumors were squamous cell carcinoma (n=15), acinic cell carcinoma (n=9), and mucoepidermoid carcinoma (n=6). Twenty patients (45.5%) received postoperative radiation therapy. Complications included: surgical site necrosis (13%), hematoma (4.3%), and infection (2.2%). Overall incidence of malignant recurrence was 4.4% with a mean time of follow-up of 10.3 (range 0 – 77.3) months. Incidence of malignant recurrence in the fat graft reconstruction subset was 0% with a mean follow-up of 9.8 (range 0.2 – 49.3) months. There was no association with use of fat graft and recurrence (p>0.05).
Conclusion: Parotidectomy defects for malignant neoplasms can be reconstructed with fat graft transfers with no impact on surveillance for disease recurrence.
-

Avoidance of Maxillary Swing for Nasopharyngectomy via Combined Open Lateral and Endoscopic Approach
S. Hamad Sagheer, BS; Brian Swendseid, MD; Joseph M. Curry, MD; Mindy Rabinowitz, MD; Gurston Nyquist, MD; Marc R. Rosen, MD; James Evans, MD; and Adam J. Luginbuhl
Objectives: Nasopharyngectomy performed via a solely endoscopic approach has limitations in access and feasibility, particularly regarding management of the carotid artery. To address these limitations, we report three cases with one cadaver dissection where nasopharyngectomy was performed via a combined open lateral an endoscopic approach. We highlight the benefits and technical considerations for this operative technique.
Study Design: Case Series
Methods: Patients diagnosed with recurrent nasopharyngeal carcinoma (NPC) that underwent combined open lateral and endoscopic nasopharyngectomy from 2016-2020 were analyzed. A cadaver dissection was also performed.
Results: We present the details of the approach and follow-up in three patients with recurrent nasopharyngeal carcinoma. Briefly, a preauricular incision is extended down to the neck. The zygoma and mandibular ramus can be removed and replaced if required. V3, the pterygoid plates and the eustachian tube can be resected or mobilized. The carotid artery may be identified proximally in the neck and traced to the skull base, where the carotid canal may be drilled to the level of the foramen lacerum and protected with a pledget. Then, tumor mucosal cuts are made via an endoscopic endonasal approach and connected to the lateral exposure. No carotid artery injuries occurred.
Conclusion: The combined open lateral approach and endoscopic nasopharyngectomy technique is a useful technique in salvage patients. It provides excellent control of major vessels, adequate access to the carotid canal, V3, and remainder of the skull base, and cervical protection.
-

Gastric Pepsin in Post-Tympanostomy Tube Otorrhea
Jill N. D'Souza, MD; Erin Fields, PA-C; Zhaoping He, PhD; and Robert O' Reilly, MD
Introduction
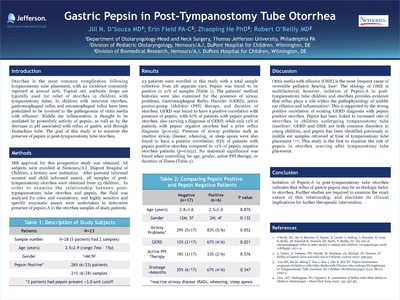
Otorrhea is the most common complication following tympanostomy tube placement, with an incidence commonly reported at around 20%. Topical otic antibiotic drops are typically used for relief of otorrhea in children with tympanostomy tubes. In children with recurrent otorrhea, gastroesophageal reflux and extraesophageal reflux have been postulated to be involved in the pathogenesis of otitis media with effusion1. Middle ear inflammation is thought to be mediated by proteolytic activity of pepsin, as well as by the decrease in pH associated with reflux of gastric acid through Eustachian tube. The goal of this study is to examine the presence of pepsin in post-tympanostomy tube otorrhea.
Poster presented at: Pennsylvania Academy of Otolaryngology in Bedford PA.
-

Dual Kidney Allocation Score: A Novel Algorithm Utilizing Expanded Donor Criteria for the Allocation of Dual Kidneys in Adults
Jill N. D'Souza, MD; Katherine McKee-Cole, MD; Abigail Strang, MD; Patrick Barth, MD; Aaron Chidekel, MD; and Udayan Shah, MD
Abstract:
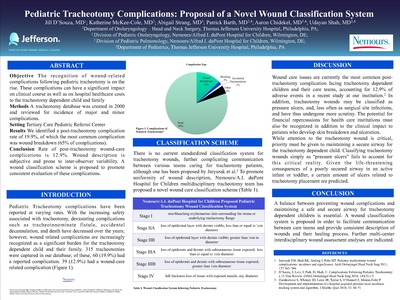
Objective The recognition of wound-related complications following pediatric tracheotomy is on the rise. These complications can have a significant impact on clinical course as well as on hospital healthcare costs to the tracheotomy dependent child and family
Methods A tracheotomy database was created in 2000 and reviewed for incidence of major and minor complications.
Setting Tertiary Care Pediatric Referral Center
Results We identified a post-tracheotomy complication rate of 19.9%, of which the most common complication was wound breakdown (65% of complications).
Conclusion Rate of post-tracheotomy wound-care complications is 12.9%. Wound description is subjective and prone to inter-observer variability. A wound classification scheme is proposed to promote consistent evaluation of these complications.
-

Cerebrospinal fluid leak after microvascular reconstruction of large craniofacial defects with orbital exenteration
Kurren Gill, BA; David Hsu, MD; Patrick Tassone, MD,; John Pluta, MD; Gurston G. Nyquist, MD; Howard Krein, MD, PhD; Jurij Bilyk, MD; Ann P. Murchison, MD; Alfred Iloreta, MD; James J. Evans, MD; Ryan N. Heffelfinger, MD; and Joseph M. Curry, MD
Abstract
Objectives: To assess risk factors for cerebrospinal fluid (CSF) leak after microvascular reconstruction of extensive cranio-orbitofacial resection with orbital exenteration (CFOE).
Study Design: Retrospective Case Series
Methods: 70 consecutive patients at a tertiary hospital underwent 76 procedures with microvascular reconstruction of CFOE defects. Patients were stratified by extent of skull base exposure and presence or absence of dural resection. Patients with exposure of the orbital apex and roof alone were classified as minimal skullbase exposure (MSE, n=32). Those with exposure beyond the orbital apex and roof were classified as significant skullbase exposure (SSE, n=38), including those with dural resection (n=23). The main outcome measure was incidence of postoperative CSF leak according to univariate and multivariate analysis of risk factors.
Results: Five patients developed a postoperative CSF leak, and 3 required operative management. All 5 were SSE with dural resection and had middle fossa exposure, previous radiation and 4 had previous surgery. None of the MSE group or SSE without dural resection or SSE with anterior fossa exposure alone developed a CSF leak. Multivariate analysis revealed middle fossa exposure to be the only significant predictor of CSF leak (p=0.03). The overall complication rate was 31.6%. Major complications were greater in the SSE group (p=0.05).
Conclusion: Middle fossa exposure increases the risk of CSF leak in microvascular reconstruction of CFOE defects.
-

Thyroid Cancer Metabolism: A Review
Kurren Gill, BA; Patrick Tassone, MD,; James Hamilton, MD; Nikolaus Hjelm, MD; Adam J. Luginbuhl, MD; David Cognetti, MD; Madalina Tuluc, MD; Ubaldo E. Martinez-Outshoorn, MD; Jennifer Johnson, MD; and Joseph Curry, MD
Abstract
Metabolic dysregulation within the tumor microenvironment (TME) is critical to the process of tumorigenesis in various cancer types. Thyrocyte metabolism in papillary and anaplastic thyroid cancer, however, remains poorly characterized, and studies analyzing the role of multicompartment metabolism in thyrocyte oncogenesis are sparse. We present a review of the current knowledge on cellular metabolism in non-cancerous and cancerous thyroid tissues, focusing on the monocarboxylate transporters MCT1 and MCT4, and on a transporter of the outer mitochondrial membrane TOMM20. Understanding the metabolic phenotype of tumor cells and associated stromal cells in thyroid cancer can have profound implications on the use of biomarker staining in detecting subclinical cancer, imaging as it relates to expression of various transport proteins, and therapeutic interventions that manipulate this dysregulated tumor metabolism to halt tumorigenesis and eradicate the cancer. Future studies are required to confirm the prognostic significance of these biomarkers and their correlation with existing staging schemas such as the AGES, AMES, ATA and MACIS scoring systems.
.
-

Benefits of a surgical safety checklist for otolaryngology patients
Lindsay A. Goodstein, MD; Nadia K. Mostovych, MD; Michael B. Hall, MD; David Hsu, MD; David Cognetti, MD; and Maurits S. Boon, MD
Introduction
The volume and complexity of knowledge today has exceeded any single individual's ability to manage it consistently without error despite advances in technology, years of training, and specialization of functions and responsibilities. Checklists have been employed since the 1930s in aviation and high-risk industries to prevent accidents caused by human error. Only recently has their use been introduced to surgery after the World Health Organization (WHO) heightened awareness of the significant number of deaths, about a half million worldwide, that occur each year as a result of avoidable surgical error.1 With over 275,000 surgical procedures performed daily, an emphasis on perioperative safety is a necessity.2
The WHO developed the first surgical safety checklist for use in the operating room in 2007. Since implementation, the checklist has reduced morbidity and mortality by over 30%.3 Subsequently, many hospitals have adapted and implemented checklists to improve patient outcomes. Moreover, the Centers for Medicare & Medicaid Services (CMS) recommended the use of surgical safety checklists as a quality measure in 2016. Thomas Jefferson University Hospital (TJUH) implemented a formalized time out procedure based on the WHO checklist with assistance from the LifeWings project for patient safety in 2013.
The original objective of the WHO checklist was for use in all settings where surgery takes place. However, there is increasing consensus that checklists should be customized to meet the needs of different surgical specialties in order to ensure optimal safety.4,5 The TJUH iteration of the WHO surgical safety checklist is centered on a time out procedure that occurs prior to incision, but after administration of anesthesia. Otolaryngology patients and operations can be complex, requiring advance communication and planning, prior to bringing each patient to the operating room, to safely secure the airway and obtain the necessary surgical equipment.
Our objectives were 1) to assess perceptions of operative safety and teamwork among nurses, otolaryngologists and anesthesiologists; and 2) to implement a preoperative surgical safety checklist to improve perioperative teamwork and communication.
Poster presented at Thomas Jefferson University House Staff Quality and Safety Poster Day.
-

Benefits of Wireless Telephone Technologies for Bilaterally Implanted Adults
Louisa Liang, Au.D. and Paula Marcinkevich, Au.D.
Introduction
Cochlear implant (CI) recipients often have difficulty conversing on the telephone, particularly in noise. Successful use of landline and cellular telephones also can be limited because of less-than-optimal phone placement with respect to the sound processor microphone. One solution for recipients of Advanced Bionics cochlear implants may be the use of new streaming technologies from Phonak to improve the ability to talk on the phone. In addition to reducing interference caused by noise, use of these technologies is not strictly placement-dependent and also allows bilateral/bimodal recipients to take advantage of hearing with two ears.
The primary objective of this study was to assess the telephone communication benefits of Phonak’s telephone technologies that stream full bandwidth audio signals from ear to ear wirelessly. In addition, a questionnaire for the CI recipient and also their communication partner (when appropriate) evaluated sound quality, ease of use, and perceived benefit for each accessory/technology.
-

The Effects of Formalized Team Training on Key Patient Outcomes in an Otolaryngology- Head and Neck Surgery Residency
Natalie Vercillo, MD; Adam Vasconcellos, MD; David Cognetti, MD; and Maurits Boon, MD
BACKGROUND
- Errors in medical care have consistently been linked to communication failures among team members. TeamSTEPPS® is a team training system which was co-developed by the Department of Defense and the Agency for Healthcare Research and Quality (AHRQ) which provides a full curriculum of ways to improve patient safety through four main skills: communication, mutual support, leadership and situation monitoring1.
- Training in these skills through TeamSTEPPS® has been shown to improve patient safety and outcomes by reducing destructive barriers within the healthcare field such as poor communication, conflicts, ambiguous responsibilities of each team member, hierarchical constraints and work overload. In addition to providing a full curriculum to create efficient, highly functioning teams, TeamSTEPPS® provides support for implementation into one’s own healthcare system. Numerous studies have shown positive effects of team training with TeamSTEPPS®.
- We provide the various steps taken by our department to proactively improve patient care so other institutions can use as this as a model for implementation of TeamSTEPPS®.
Poster presented at Thomas Jefferson University Quality and Safety Day.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}