

Files
Download Poster (9.1 MB)
Description
Introduction: Spinal dural arteriovenous fistula (SDAVF) is an abnormal connection between the arterial and venous system creating an increase in blood flow and pressure into the spinal veins1 at an estimated frequency of 5-10 cases per million per year.2 Activities that increase intrathoracic and venous pressure such as Valsalva, abdominal compression and steroids2 can lead to a venous infarction, subarachnoid hemorrhage, paraplegia or tetraplegia.3 SDAVF is difficult to diagnose as it presents similarly to other neurologic disorders, but if diagnosed early, deficits can be prevented and reversed with intervention.1
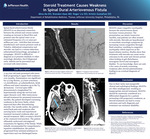
Case Description: A 54-year-old male presented with lower limb progressing to upper limb weakness over months. Examination was significant for 2/5 hip flexion, 3/5 knee extension, 1/5 dorsiflexion, 4/5 plantarflexion, brisk reflexes and intact sensation up to the T4 dermatome. Cervical spine MRI demonstrated a longitudinal T2 hyperintensity along the cervical and upper thoracic cord. After intravenous steroid treatment for presumed transverse myelitis, the patient developed worsening weakness in the lower limbs, which improved days after discontinuing steroids. One month earlier, the patient noted back pain and weakness after carrying heavy tools and experienced transient increased weakness after oral steroid treatment. MRA revealed a SDAVF at the craniocervical junction. The patient ultimately underwent retrosigmoid craniotomy for ligation of the fistula. While initially recommended for comprehensive inpatient rehabilitation, the patient progressed from minimal assistance to supervision and was discharged home.
Discussion: SDAVFs cause congestive myelopathy because the arteriovenous shunt increases venous pressure. The presentation can mimic transverse myelitis, and patients are often treated with steroids. Steroids are hypothesized to exacerbate neurologic symptoms by increasing venous congestion through fluid retention, resulting in congestive myelopathy which improves as the hypervolemia resolves. Studies show that treatment with steroids can cause worse outcomes in the acute and chronic period when looking at gait disturbance, neurogenic bowel and neurogenic bladder. To our knowledge, there are only a few cases of acutely worsening weakness after steroid administration leading to an eventual diagnosis of SDAVF.
Conclusion: Due to their rarity and nonspecific clinical and radiological findings, SDAVFs are often misdiagnosed, resulting in inappropriate steroid treatment. SDAVFs should be cautiously considered as a differential diagnosis for a patient presenting with progressive weakness, as steroid treatment can lead to worse outcomes and early diagnosis and treatment can minimize disability.
Publication Date
2-15-2023
Keywords
subdural arteriovenous fistula, SDAVF, spinal cord injury, SCI
Disciplines
Medicine and Health Sciences | Rehabilitation and Therapy
Recommended Citation
Na, DO, Mina; Kase, MD, Brandon; Liu, DO, Roger; and Gustafson, DO, Kristin, "Steroid Treatment Causes Weakness in Spinal Dural Arteriovenous Fistula" (2023). Department of Rehabilitation Medicine Posters. 14.
https://jdc.jefferson.edu/rmposters/14

Comments
Presented at the 2023 Association of Academic Physiatrists Annual Meeting.